Fascia is a thin film of tissue membrane that covers muscles, bones, blood vessels, and even nerves.
Lack of consistent terminology within health and medicine in relation to fascia causes many problems in the health and physical therapy. Since fascia represents a topic of growing interest worldwide, it should be a priority to reduce ambiguity in fundamental terms so that this field of research can properly advance. For example, the lack of common definitions and nomenclature hinders communication between those involved in the process of diagnosis and treatment of pelvic pathologies in everyday practice.
The usage of the terms superficial fascia and deep fascia is considered incorrect by the Federative International Committee on Anatomical Terminology (FICAT) because histological terminology referring to layers of the connective tissue varies too much internationally to be generalized by these two terms
The FICAT broadly defines fascia as sheaths.
The First International Fascia Research Congress (2007) formulated a comprehensive definition of fascia as the soft tissue component of the connective tissue system, emphasizing its uninterrupted, three-dimensional web-like extensions and highlighting its functional attributes. The broad nature of these two definitions is controversial, and not all of the tissues have been widely accepted into common usage. Thus, a consistent terminology to classify and categorize fascia has not been formally established and accepted internationally.
A more recent ontology highlights the importance of two functional forms of fascia, connecting and disconnecting, for which fiber orientation and descriptions of fascia’s role in proprioception are key justifications for each category.
These 4 categories were developed based primarily on the functional properties of fasciae, with further observations from the literature on gross anatomical, histological and biomechanical features, and terms unique to each category. Such a classification system based on functional properties of fasciae may have more relevance to the clinical experiences of manual therapists.
4 categories of fascia
Linking Fascia
The linking category is predominantly dense regular parallel ordered unidirectional connective tissue proper with a significant amount of collagen type I.
This category is subdivided into dynamic and passive divisions.
The dynamic division includes major fascial groups more significantly related to movement and joint stability, and characterized by higher concentrations of contractile and proprioceptive fibers. The dynamic division is composed of fasciae of muscles (investing layer, fascia of individual muscle), and fasciae of the trunk.
The passive division is acted on by other extramuscular tissues to maintain continuity throughout the body or form tunnels and sheaths. The passive division incorporates fasciae of muscles (muscle sheaths), fasciae of the head and neck, fasciae of limbs, aponeuroses, tendinous arches, and retinaculae. This group can act as muscular insertion points, such as the epicranial aponeurosis, and as joint linkages and tendinous arches ultimately providing proprioceptive information when tension is exerted.
Fascicular fascia
2. Fascicular fascia forms adaptable tunnels which bundle vessels as well as fascicles within muscle, tendon, bone and nerves. Fascicular fascia plays an important role in organization, transport, strength and locomotion. This category is organized as a mixture of both loose and dense regular multidirectional connective tissues. Fascicular fascia of the muscle comprises three distinct layers of IMCT: epimysium surrounding whole muscles, perimysium separating fascicles or bundles of muscle fibers within the muscle, and endomysium covering the individual muscle fibers
Types I and III collagen are the major components of these tissues with lesser amounts of Types V, VI, XII, and XIV.
Compression Fascia
Compression fascia is a mixture of dense regular woven and multidirectional parallel ordered connective tissue layers that ensheath whole limbs to create a stocking effect. This fascial category plays an important role in locomotion and venous return due to its influence on compartmental pressure, muscle contraction and force distribution.
For example, the crural fascia is composed of two or three layers of parallel ordered collagenous fiber bundles, each layer being separated by a thin layer of loose connective tissue.he spatial orientation of the collagen fibers changes from layer to layer within the compression fascia.
The presence of loose connective tissue interposed between adjacent layers permits local sliding, allowing the single layers to respond more effectively. Examples of this type of fascia are observed in the limbs and are observed as fascia lata, crural fascia, brachial fascia, and antebrachial fascia.
Separating Fascia
Separating fascia is generally loose connective tissue and dense irregular fusocellular connective tissue.
It is difficult to gain an appreciation for the true appearance of fascia, aside from basic structure, in embalmed cadavers. Direct observation of fascia’s appearance and behavior in a living, hydrated body, has been conducted with recent fluoroscopic imaging under the skin of the dorsal forearm, shedding new light on how this sliding collagenous system works.
These observations demonstrate that fascia incorporates a water dense vacuolar system able to slide independent of the rate of contraction in muscle around it and able to conduct structures like capillaries throughout sections of myofascia.
This fascia class is a complex connective tissue matrix, ensheathing everything from body cavities to individual organs. It separates, supports, and compartmentalizes organs and regions in order to maintain proper structural and functional relationships throughout the body. This group of fascia has a unique appearance and texture upon observation, ranging from transparent woven sheets to a fuzzy cotton-like consistency.
Deep sustained pressure may be necessary for manual practitioners to affect this fascial tissue.
Fascia doesn’t have a beginning and end like muscles.
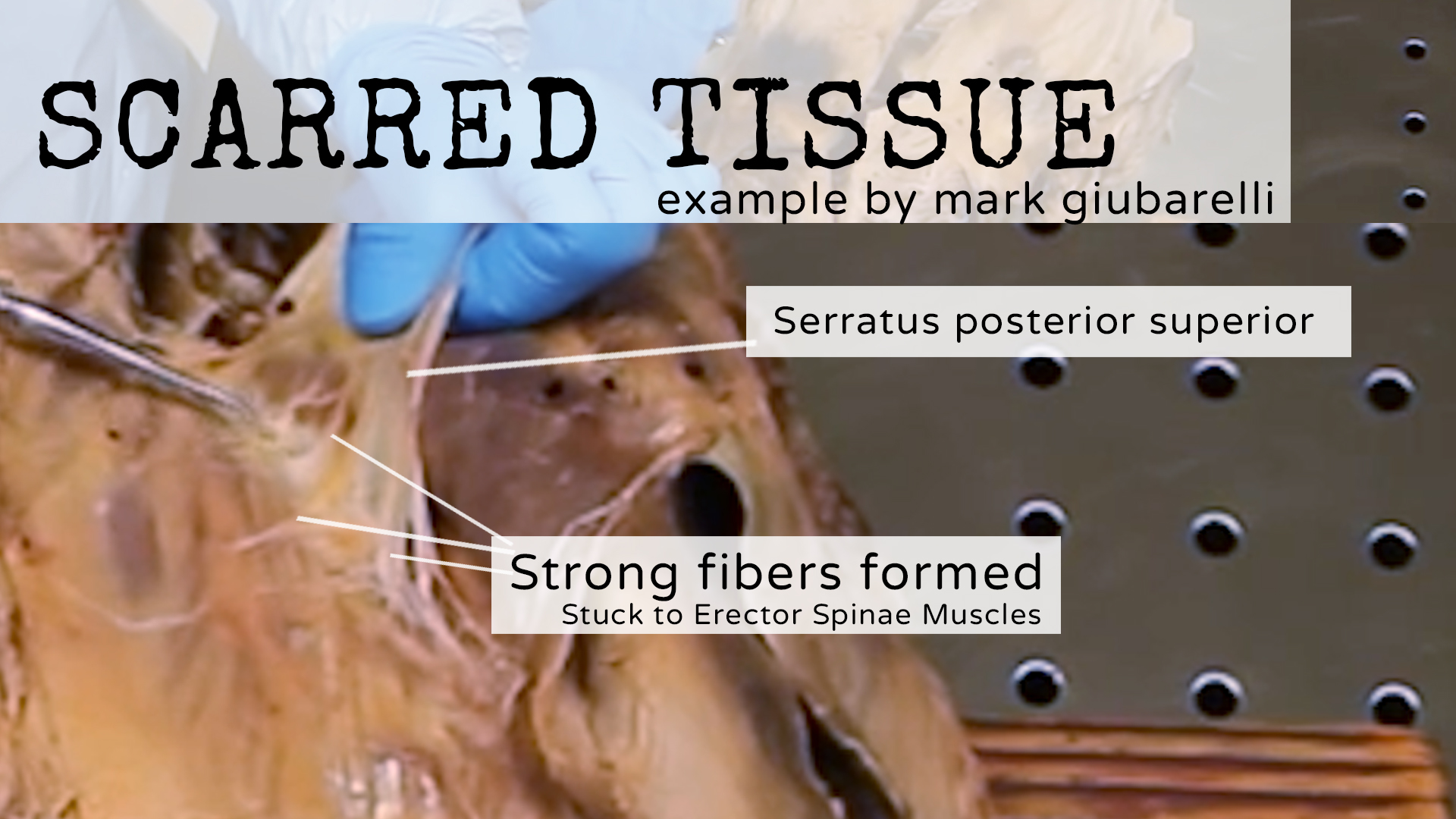
Picture of Scarred Tissue Example